Well Child Exam Form - Infancy: 2 Months Page 2
ADVERTISEMENT
 1
1 2
2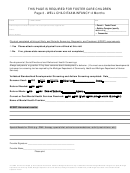 3
3 4
4Page 2 - WELL CHILD EXAM-INFANCY: 2 Months - Developmental Surveillance
(This page may be used if not utilizing a Validated Developmental Screener)
DATE
PATIENT NAME
DOB
Developmental Questions and Observations
Ask the parent to respond to the following statements about the infant:
Yes
No
□
□
Please tell me any concerns about the way your baby is behaving or developing:
________________________________________________________________
□
□
My baby looks at me and listens to my voice.
□
□
My baby quiets when picked up.
□
□
My baby is sleeping well.
□
□
My baby is eating well, sucking well.
□
□
My baby makes cooing sounds.
□
□
My baby lifts his/her head while on tummy.
Ask the parent to respond to the following statements:
Yes
No
□
□
I am sad more often than I am happy.
□
□
I have more good days with my baby than bad days.
□
□
I have people who help me when I get frustrated with my baby.
Provider to follow up as necessary
Developmental Milestones
Always ask parents if they have concerns about development or behavior. (You may use the following screening list, or a
standardized developmental instrument or screening tool).
Infant Development
Parent Development
Coos and vocalizes reciprocally
Yes
No
Looks at infant
Yes
No
Smiles responsively
Yes
No
Picks up and soothes infant or comforts
Yes
No
baby effectively
Follows to midline
Yes
No
Are parent and baby interested in and
Yes
No
responsive to each other?
Is attentive to voices, sounds, visual stimuli
Yes
No
Does parent seem depressed, angry, tired,
Yes
No
overwhelmed, or uncomfortable?
Some head control in upright position
Yes
No
Shows pleasure interacting w/parent
Yes
No
Please note: Formal developmental examinations are recommended when surveillance suggests a delay or abnormality, especially when the opportunity for
continuing observation is not anticipated. (Bright Futures: Guidelines for Health Supervision of Infants, Children, and Adolescents)
Additional Notes from pages 1 and 2:
Staff Signature: ________________________________ Provider Signature: ___________________________________
This HME form was developed by the Institute for Health Care Studies at Michigan State University in collaboration with the Michigan Medicaid managed care plans, Michigan
Department of Community Health, Michigan Department of Human Services, Michigan Association of Health Plans, and Michigan Association of Local Public Health.
Updated – 4/2011
ADVERTISEMENT
0 votes
Related Articles
Related forms










Related Categories
Parent category: Medical