Application To Reinstate A Former Tier 1 Or 2 Membership
Download a blank fillable Application To Reinstate A Former Tier 1 Or 2 Membership in PDF format just by clicking the "DOWNLOAD PDF" button.
Open the file in any PDF-viewing software. Adobe Reader or any alternative for Windows or MacOS are required to access and complete fillable content.
Complete Application To Reinstate A Former Tier 1 Or 2 Membership with your personal data - all interactive fields are highlighted in places where you should type, access drop-down lists or select multiple-choice options.
Some fillable PDF-files have the option of saving the completed form that contains your own data for later use or sending it out straight away.
ADVERTISEMENT
 1
1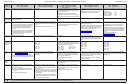 2
2 3
3Application to Reinstate a
Receipt Date
Former Tier 1 or 2 Membership
in Accordance with Section 645
Office of the New York State Comptroller
New York State and Local Retirement System
RS 5506
Employees’ Retirement System
Police and Fire Retirement System
Office Use Only
(Rev. 8/13)
110 State Street, Albany, New York 12244-0001
Complete and return this application only if you previously held a membership in any of the retirement systems
listed below, with a date of membership prior to July 26, 1976.
You must be a current member of the Retirement System. Retirees are not eligible for this benefit.
Please complete pages 1 and 4 of this form. Pages 2 and 3 provide a comparison of benefits for members covered under
regular plans. If you are covered by a 20 or 25 year plan you should contact the Retirement System if you have any questions.
Please read this information and if you have any questions call our Information Office toll free at 1-866-805-0990, Albany area
474-7736 or contact us via email at nyslrsinfo@osc.state.ny.us.
SOCIAL SECURITY # _________________________________ DATE OF BIRTH _____________________________
CURRENT RETIREMENT SYSTEM REGISTRATION # ____________________________________________________
LAST NAME ______________________________________ FIRST ______________________________ M.I. _______
STREET ADDRESS ________________________________________________________________________________
CITY ______________________________________________ STATE _________ ZIP CODE ____________________
(
)
(
)
WORK PHONE NUMBER: ________________________ HOME PHONE NUMBER _____________________________
EMAIL ADDRESS __________________________________________________________________________________
FORMER MEMBERSHIP INFORMATION:
PLEASE CHECK THE APPROPRIATE FIRST FORMER RETIREMENT SYSTEM YOU WERE A MEMBER OF:
q
New York State Teachers’ Retirement System
q
New York City Board of Education Retirement System
q
New York State Employees’ Retirement System
q
New York City Teachers’ Retirement System
q
New York State Police and Fire Retirement System
q
New York City Police Pension Fund
q
New York City Employees’ Retirement System
q
New York City Fire Pension Fund
PLEASE COMPLETE THE FOLLOWING (if known):
Former Registration Number: ____________________________
Date of Membership: ______________________
Former Name (if applicable): ________________________________________________________________________
Have you received credit for this former membership in any other retirement system?
Yes ___
No ___
If Yes, what Retirement System: _______________________________________________________________________
Are you receiving or eligible to receive a retirement benefit based on this service?
Yes ___
No ___
PREVIOUS PUBLIC EMPLOYMENT INFORMATION:
Name of Employer
Name of Dept.
Title of Position
From
To
or Agency
Mo.
Day
Year
Mo.
Day
Year
ADVERTISEMENT
0 votes
Related Articles
Related forms







 Endorsement Deficiency Form")


Related Categories
Parent category: Legal