Form Dwc-01 - Employer'S First Report Of Alleged Occupational Injury, Disease Or Fatality Page 13
Download a blank fillable Form Dwc-01 - Employer'S First Report Of Alleged Occupational Injury, Disease Or Fatality in PDF format just by clicking the "DOWNLOAD PDF" button.
Open the file in any PDF-viewing software. Adobe Reader or any alternative for Windows or MacOS are required to access and complete fillable content.
Complete Form Dwc-01 - Employer'S First Report Of Alleged Occupational Injury, Disease Or Fatality with your personal data - all interactive fields are highlighted in places where you should type, access drop-down lists or select multiple-choice options.
Some fillable PDF-files have the option of saving the completed form that contains your own data for later use or sending it out straight away.
ADVERTISEMENT
 1
1 2
2 3
3 4
4 5
5 6
6 7
7 8
8 9
9 10
10 11
11 12
12 13
13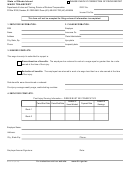 14
14 15
15 16
16 17
17 18
18State of Rhode Island
REPORT OF EARNINGS
Department of Labor and Training, Division of Workers' Compensation
Insurer File No.
Phone (401) 462-8100 TDD (401) 462-8006
1. EMPLOYEE INFORMATION:
2. CLAIM ADMINISTRATOR:
SSN
FEIN
Name
Name
Address
Address
City, State, Zip
City, State, Zip
Phone
Phone
Ext.
This report covers the time period from:
to:
PRESENT
3. NOTICE TO EMPLOYEES RECEIVING WORKERS' COMPENSATION:
If you are receiving weekly workers’ compensation benefits, YOU MUST REPORT ANY EARNINGS YOU RECEIVE TO THE CLAIM ADMINISTRATOR
THAT IS PAYING YOUR BENEFITS. “Earnings” include any cash, wages, or salary received from self-employment or from any employer other than the
employer where you were injured. Earnings also include commissions, bonuses, and the cash value for all payments received in any form other than
cash (for example: a building custodian receiving a rent-free apartment).
Your endorsement on a benefit check or deposit of the check into an account is your statement that you are entitled to receive workers’ compensation
benefits. Your signature on a benefit check is a further affirmation that you have made no false claims or statements or concealed any material fact
regarding your workers’ compensation claim.
You must report any work for any business or person, even if the business or person lost money or if profits or income were reinvested or paid to others.
If you performed any duties for any business or person for which you were not paid, you must show a rate of pay of what it would have cost the employer
to hire someone to perform the work you did, even if your work was for yourself, a relative, or friend.
You are NOT entitled to workers’ compensation benefits for any time you are imprisoned as a result of a criminal conviction.
4. Employee Complete:
1. Did you receive earnings or payments during the above period?
State YES or NO:
2. Did you perform non-paid work activities during the above period? State YES or NO:
If you answered NO to BOTH questions, sign, date and return the form to the CLAIM ADMINISTRATOR above.
If you answered YES to EITHER question, complete the following:
Employer Name
Self-Employed?
Yes
No
Address
Nature of business
City
State
Zip Code
Phone
5. Earnings Received:
Report pre-tax earnings. Include any cash, bonus, commission, and the cash value of any payment
received in any form other than cash. Attach additional pages if necessary.
Date Earned:
Amount:
Date Earned:
Amount:
Date Earned:
Amount:
Date Earned:
Amount:
Failure to report earnings as defined will subject you to criminal prosecution and civil liability including the suspension or forfeiture of your
benefits. This form MUST BE SIGNED, DATED and returned to the Claim Administrator -- EVEN IF YOU HAVE NO EARNINGS.
Employee Signature:
Date:
Witness Signature:
Date:
For instructions visit our web site:
DWC-25 (01/03)
ADVERTISEMENT
0 votes
Related Articles
Related forms










Related Categories
Parent category: Business