Form Dwc-01 - Employer'S First Report Of Alleged Occupational Injury, Disease Or Fatality Page 12
Download a blank fillable Form Dwc-01 - Employer'S First Report Of Alleged Occupational Injury, Disease Or Fatality in PDF format just by clicking the "DOWNLOAD PDF" button.
Open the file in any PDF-viewing software. Adobe Reader or any alternative for Windows or MacOS are required to access and complete fillable content.
Complete Form Dwc-01 - Employer'S First Report Of Alleged Occupational Injury, Disease Or Fatality with your personal data - all interactive fields are highlighted in places where you should type, access drop-down lists or select multiple-choice options.
Some fillable PDF-files have the option of saving the completed form that contains your own data for later use or sending it out straight away.
ADVERTISEMENT
 1
1 2
2 3
3 4
4 5
5 6
6 7
7 8
8 9
9 10
10 11
11 12
12 13
13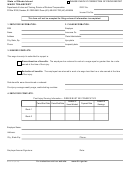 14
14 15
15 16
16 17
17 18
18State of Rhode Island
PLEASE CHECK IF CORRECTION OF PRIOR REPORT
MUTUAL AGREEMENT
DWC No.
Department of Labor and Training, Division of Workers' Compensation
PO Box 20190, Cranston, RI 02920-0942
Phone (401) 462-8100 TDD (401) 462-8006
Insurer File No.
1. EMPLOYEE INFORMATION:
2. CLAIM INFORMATION:
SSN
Employer
Name
Insurance Co.
Address
Claim Administrator
City, State, Zip
Injury date
Phone
Incapacity date
This form may be used pursuant to Rhode Island General Law § 28-35-6(b) to amend a
Memorandum of Agreement, Order or Decree regarding a Workers' Compensation claim.
This form cannot be used for commencement or termination of weekly benefits.
YOU MUST ATTACH A COMPLETED REPORT OF INDEMNITY PAYMENT (DWC-22) TO THIS MUTUAL AGREEMENT.
3. INDICATE THE ACTION(S) OF THIS MUTUAL AGREEMENT:
Change total average weekly wage from
$
to $
Change weekly spendable base wage to
$
as of
(date)
Change weekly compensation rate to
$
as of
(date)
Single
Married
Change marital status to
as of
(date)
Change maximum number of exemptions to
as of
(date)
Change number of dependents to
as of
(date)
Change nature of injury and/or affected body part to
Modify from total to partial incapacity as of
(date)
Modify from partial to total incapacity as of
(date)
Suitable Alternative Employment (Attach SAE Offer)
as of
(date)
Other (Specify)
DO NOT USE THIS FORM FOR A SPECIFIC INJURY (DISFIGUREMENT, LOSS OF USE, HEARING LOSS);
USE THE REPORT OF SPECIFIC PAYMENT (DWC-51).
Employee Signature:
Date:
Employer/Insurer Signature:
Date:
For instructions visit our web site:
DWC-24 (01/03)
ADVERTISEMENT
0 votes
Related Articles
Related forms










Related Categories
Parent category: Business