Income Tax Refund Request Form - City Of Springfield, Ohio
ADVERTISEMENT
 1
1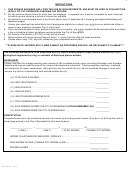 2
21
INCOME TAX REFUND REQUEST
CITY OF SPRINGFIELD, INCOME TAX DIVISION
Employer
76 EAST HIGH STREET
Account #_______________
SPRINGFIELD, OHIO 45502
(FOR OFFICE USE ONLY)
PHONE (937) 324-7357
THIS FORM IS INTENDED ONLY FOR THE USE OF NON-RESIDENTS, AND MUST BE USED IN
CONJUNCTION WITH A CITY OF SPRINGFIELD INCOME TAX RETURN.
PLEASE REVIEW INSTRUCTIONS ON PAGE 2 BEFORE COMPLETING FORM
PART A
Phone #
Name
( print first name, middle initial, last name )
Email Address
Present Address
( street, apt # )
Social Security #
( city, state and zip code )
Address During Period Covered by Claim, if different from present address:
From
To
( street, apt # )
( city and zip code )
TAX YEAR __________
PART B
-
Employer Name
Location Worked
Taxable
x 2%
Amount
= Refund
City Income
Tax Due
Withheld
Amount
( enter this amount
( enter this amount
( enter this amount
( enter this amount on
on line 6 of return )
on line 1 of return )
on line 4 of return )
line 15 of return )
Please provide a clear and concise explanation of reason for refund:
PART C
EMPLOYER VERIFICATION AND AFFIDAVIT: I hereby certify that __________________(employee name) was
employed by the undersigned during the period for which said employee makes claim for refund and that the amount of
$___________________ was withheld in excess of his/her liability based on the above stated facts and calculations;
and that no portion of said tax withheld has been or will be refunded directly to the employee, and no adjustment in
withholding remittance has been or will be made. I further declare that the information contained herein is true and
correct to the best of my knowledge and belief and that I am authorized to provide this information.
Authorized Name _____________________________________ Title ______________________________________
( print first name, middle initial, last name)
Authorized Signature __________________________________ Date _____________________________________
Name of Employer ____________________________________ Phone ____________________________________
ADVERTISEMENT
0 votes
Related Articles
Related forms










Related Categories
Parent category: Financial